Dipendra Tiwari wants to provide home health care to refugees in Louisville in a language they understand. But Kentucky won’t let him because it says that service isn’t needed. How can that be? The answer is a government permission slip called a certificate of need.
Nearly 100,000 Nepali speakers have been welcomed to the United States after ethnic tensions forced them out of their homes in the Himalayan country of Bhutan. Thousands of these refugees resettled in Louisville. And, just like anyone else, they need health care as they age. This situation gave Dipendra, a native Nepali speaker, an idea for a valuable service: a home health care agency catering to the refugee population, offering service in their own language. So, Dipendra formed Grace Home Care and paid a $1,000 fee to submit his plan to the state.
That’s when things went wrong. A $2 billion health care conglomerate—Dipendra’s future competitor—stormed in to argue that there was no need for another home health agency. Based on some back-of-the-envelope estimates, and ignoring the need for Nepali-language care that Dipendra was trying to address, Kentucky agreed. It refused to issue a certificate of need and rejected Dipendra’s application.
And that’s exactly how certificates of need are supposed to work. Originating in a long-debunked effort to control costs, in practice, all they do is prevent new businesses from competing with established ones. They are why in Kentucky’s 120 counties, new home health agencies are allowed in only eight. They are why Louisville itself has only nine home health agencies for 22,000 patients. And, to be clear, they have nothing to do with ensuring health or safety (which are covered by other laws). Rather, the whole point of current CON laws is to benefit established providers by stifling competition.
But giant health care conglomerates don’t need the government to protect their business. And entrepreneurs shouldn’t lose their shot just because someone else happened to get there first.
That’s why Dipendra has teamed up with the Institute for Justice to challenge Kentucky’s CON requirement for home health agencies in federal court. The Constitution protects the right to earn an honest living free from unreasonable government interference. And it is unreasonable for Kentucky to pick winners and losers in the marketplace.
Beyond Kentucky, 17 other states require CONs for home health agencies. But with health care costs rising, the last thing the government should be doing is imposing fewer choices and higher prices. Patients and providers—not the government—are in the best position to decide what medical services are needed.
After unfavorable decisions at the district and appeals courts, Dipendra appealed to the U.S. Supreme Court, which declined to hear the case.
Case Team


Attorneys

Andrew Ward
Senior Attorney
Staff

Andrew Wimer
Director of Media Relations
Case Documents
Complaint
Order Denying Motion to Dismiss
Motion for Summary Judgment
Appeals Court Decision
U.S. Supreme Court Cert Petition
Media Resources
Get in touch with the media contact and take a look at the image resources for the case.
Andrew Wimer Director of Media Relations [email protected]





Related News

The Lhotshampas Find Refuge in the United States
In the 19th and early 20th centuries, people from Nepal emigrated to southern Bhutan in search of work. Over the decades, these Nepalese maintained their language and culture and became known as the Lhotshampas, meaning “Southerners.” Unfortunately, in the late 1980s, the Bhutanese ruling majority started an organized campaign of discrimination against this ethnic minority. Many Lhotshampas were forced out of the country and found themselves in refugee camps in Nepal.
Just over a decade ago, many of these refugees were resettled in the United States and other English-speaking countries. Thousands of Lhotshampas now call Louisville home.
The Plaintiffs: Dipendra Tiwari and Kishor Sapkota
Dipendra Tiwari came to the United States in 2008. He then earned an MBA and became a certified public accountant. He now operates a tax and accounting firm in Louisville that caters to the Nepali-speaking population.
Dipendra’s business partner is Kishor Sapkota, a home health aide from Nepal. Thinking that they could form another business catering to Louisville’s Nepali speakers, they formed Grace Home Care, Inc. They’re well aware that limited English proficiency is one of the “key barriers” for refugees.
And while Dipendra was free to open an accounting firm focused on Nepali speakers, there is just one reason he can’t provide home health care for the same people in his community: Kentucky’s CON law.
The History of CON Laws
Put simply, a certificate of need is a government authorization to compete. Unlike in most parts of the economy, in industries regulated by CONs, it is illegal to offer a new service unless a would-be entrepreneur first proves to the government that the new service is “needed.”
The earliest medical CON requirements applied only to big publicly funded facilities such as hospitals. The theory was that restricting investment to what was needed would decrease costs. Then, in the late 1960s, the American Hospital Association began campaigning for CONs nationally because they enriched hospitals by insulating them from competition.
In the 1970s, the federal government was swayed by the hospitals and started offering states financial incentives to impose CONs. 1 The lure of federal funding led every state but Louisiana to adopt them. Over time, however, the federal government realized that CONs don’t control costs and don’t improve the health care system. Congress repealed its funding in 1986. 2 Since then, a dozen states have eliminated their CON programs.

The CON in Kentucky
That reform didn’t reach Kentucky. Today, Kentucky still requires CONs for a mishmash of medical services. 3 Assisted-living residences and group homes don’t need CONs, yet home health agencies do. So, while Dipendra could open a group home without a permission slip from his competitors, he can’t do the same for home health care.
Instead, anyone who wants to open a home health agency goes through a formal review process. It begins with a 20-page application and a fee that starts at $1,000. 4 Depending on when the application is submitted, it can take three months just for review to start. Then applications are published so that existing providers have a chance to object—usually in a hearing that amounts to a full-on trial on whether a future competitor can keep the applicant out of business. And even if the CON is granted, competitors can appeal to court. 5 The process can easily cost tens of thousands of dollars just in attorney fees.
And the game is rigged from the start. That’s because entrepreneurs may offer new services only if there’s a pre-determined need in the county where they plan to operate. Those determinations are made every two years by Kentucky’s Cabinet for Health and Family Services.
For home health agencies, it comes down to clumsy arithmetic. First, Kentucky looks at how many people in different age groups are using home health care in the state. Then, using county by county population statistics, it uses the state-wide figures to guess how many people in each county need care. Finally, it subtracts out the number of patients who recently received care in each county. The resulting difference is the “need.” The process doesn’t assess the need for services that are niche or better or innovative. It is just a guess based on middle-school math.
This certificate of need scheme is designed to let existing home health agencies and hospitals expand and keep new competitors out. Only if a county has a need of 250 people or more are new home health agencies allowed. Yet existing home health agencies can expand into a county if 125 estimated people need care. And a hospital in a county can establish a home health agency there if the need is 50. The state boils it all down in a chart every year:
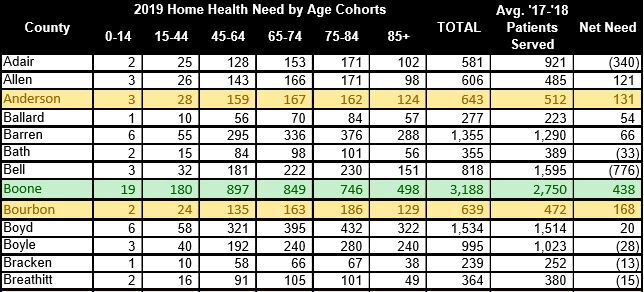
If your county is listed in green (because the need is 250 or more), new agencies are allowed. Otherwise, you’re out of luck.
But this scheme is just a handout to special interests. A major report from the Justice Department and the Federal Trade Commission found no reliable evidence that CONs benefit the public—and clear evidence that they grant anticompetitive benefits to protected business interests. The Obama administration agreed that “CON laws appear to have failed to control costs” and that “the CON process may be exploited by competitors seeking to protect their revenues.” There is even evidence that CONs lead to higher costs and worse care.
In fact, only a few years ago, Kentucky hired a national consulting firm to review health care in the state. It recommended “Suspending / discontinuing the CON program for home health agencies.” But entrenched interests objected. Hospitals, for example, argued that Kentucky should exempt hospitals’ own agencies from the CON requirement, while keeping it for everyone else. Today, the CON remains, keeping hardworking people like Dipendra from meeting the true needs of their communities.
The Legal Claims
That’s why, with help from the Institute for Justice, Dipendra is defending his rights in court. He’s bringing two legal claims.
First, everyone has the right to earn an honest living free from irrational laws. Letting giant health care conglomerates keep entrepreneurs out of business has nothing to do with protecting the public—and everything to do with protecting entrenched corporations. That is not a legitimate government interest. 6
Second, Kentucky’s CON law applies to businesses unequally. Established businesses get to operate based on a calculation from years or decades earlier; there’s no need required to stay in business. To start a business, however, depends on the number a crude formula spits out. And for some businesses, there’s no requirement at all. For example, assisted-living facilities perform services akin to home health, except they invest more capital first. If they don’t need to prove they’re needed—before investing greater capital—why should home health agencies?
After all, can you imagine this sort of “need” requirement in any other industry? Banning new supermarkets wouldn’t make groceries cheaper. In health care, like anywhere else, when an entrepreneur has a lightbulb moment, the government has no business forcing patients to keep using candles.
The Litigation Team
Dipendra and Kishor are represented by Institute for Justice Attorneys Jaimie Cavanaugh and Andrew Ward.
About the Institute for Justice
The Institute for Justice is a nonprofit public-interest law firm and the nation’s leading legal advocate for economic liberty. IJ has challenged CON laws in North Carolina, Iowa, and Virginia.
Related Cases

Montana Bans Doctors from Offering Medications to Their Patients Just to Protect Pharmacies from Competition
The vast majority of states allow patients to purchase medications directly from their prescribing doctor. For years, this practice was banned in Montana, until IJ stepped in to challenge the law and lawmakers immediately moved…

North Carolina Ophthalmologist Challenges Outdated Certificate of Need (“CON”) Law
The government should never prevent doctors from safely providing affordable health care services their patients need. But that’s exactly what North Carolina, along with 34 other states, do every day. Dr. Jay Singleton is working…

Texas Bans Doctors from Offering Medication to Their Patients Just to Protect Pharmacies from Competition
In most states, patients can purchase medication directly from the doctor prescribing it. But in Texas, doctors are banned from dispensing unless they practice in certain “rural” areas more than 15 miles from a pharmacy—a…




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}