CON Laws Increase Spending Per Service
Another primary legislative purpose behind Kentucky’s CON program is to deliver “cost-efficient” healthcare services. 1 Yet standard economic theory and common-sense dictate that reducing the supply of healthcare will have the opposite effect. As supply decreases, costs and prices typically increase.
There is no doubt that healthcare is a highly regulated market with many distortions (hidden pricing, third-party payment, etc.). Even so, there’s no reason to believe that restricting supply (another distortion) will decrease per-service spending. Instead, supply restrictions—even in regulated and distorted markets—tend to increase spending per service. 2 Additionally, because of their anti-competitive properties, CON laws seem likely to permit some degree of monopoly pricing power. This too, is likely to increase spending per service. 3 The data bear this out: the findings in the CON literature are predictable. Restricting the supply of healthcare does not decrease costs.
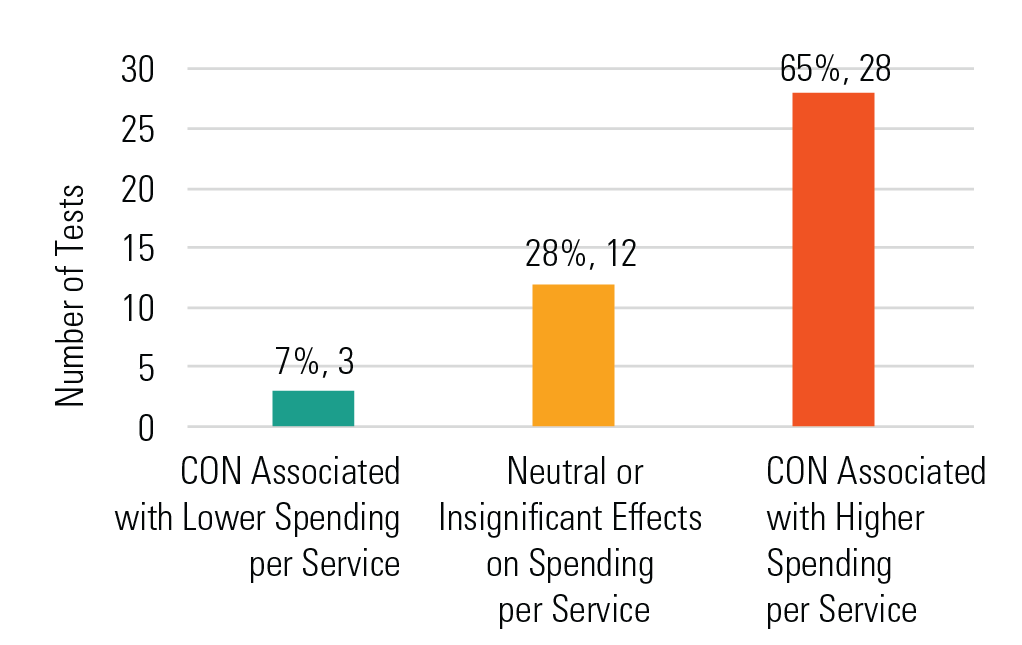
Figure 8 shows that among 43 tests, 28 (65%) tests find that CON laws are linked to higher spending per service, while a mere three tests (7%) associate them with lower spending per service.
Figure 8. Tests Assessing the Effect of CON on Spending Per Service ($/Q)
To take just a few examples:
- CON laws are associated with 10% higher variable costs in general acute hospitals, 4
- Hospital charges in states without CON laws are 5.5% lower five years after repeal, 5
- In Ohio, reimbursements for coronary artery bypass grafts fell 2.8% following repeal of CON laws; in Pennsylvania, they fell 8.8% following repeal, 6
- Acute care costs rise with the rigor of the CON program from the most resource-intense diagnoses, 7
- CON laws are associated with higher Medicaid costs for home health services, 8 and
- There is some evidence that CON is associated with higher Medicaid long-term care costs. 9
CON Laws Increase Spending Per Patient
Though economic theory offers little reason to expect CON laws to decrease spending per service, it might—as we explained at the outset of this paper—decrease spending per person or per patient. The logic is straightforward: the total amount spent per person is equal to the number of services that the person obtains, multiplied by the amount spent per service. Since CON laws are likely to decrease the number of services that people obtain while increasing the amount spent per service, its effect on total spending is theoretically ambiguous.
A CON program might, for example, lead to zero spending if it eliminated all healthcare resources (though undoubtedly this would not be socially optimal). Even this theoretical possibility, however, is unlikely. This is because healthcare services are generally found to be inelastically demanded; that is, patients will seek them out regardless of price or distance. 10
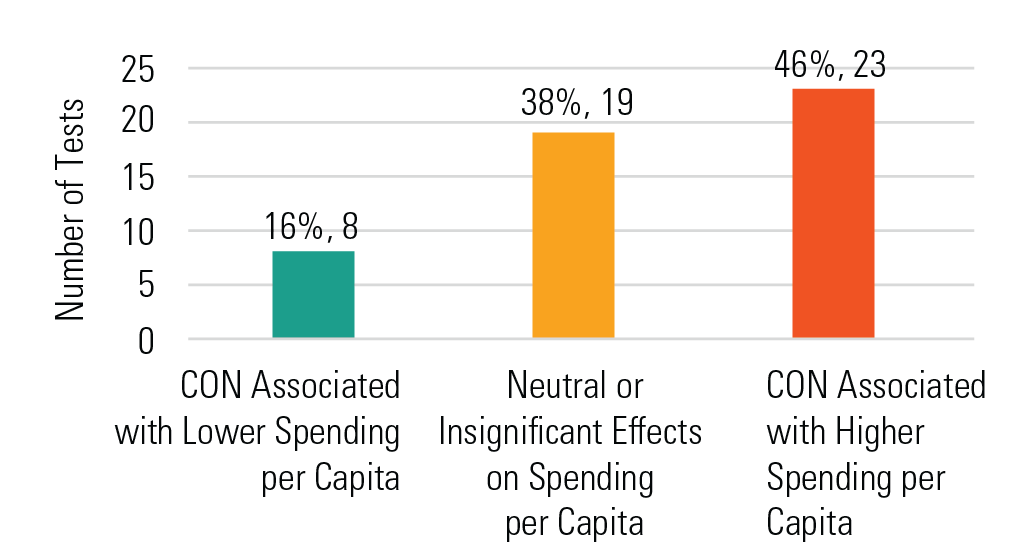
Here again, the real-world experience (shown in Figure 9) reflects standard economic theory. Among 50 tests assessing the effects of CON laws on spending per person, 46% find that CON laws are linked to higher spending per capita while only 16% associate it with lower spending per capita.
Figure 9. Tests Assessing the Effect of CON on Spending Per Capita ($/Capita)
Among these tests, researchers find:
- Hospital expenditures are 20.6% higher per capita in states with CON laws, 11
- Stringent CON programs increase hospital expenditures per admission, 12 and
- Nursing home CONs are associated with higher expenditures per resident, 13
CON Laws Increase Government Healthcare Expenditures
Increased spending translates to government payors too. These costs are ultimately borne by taxpayers. Consider:
- Medicare spending per rural beneficiary is $295 higher in states with CON laws than in states without, 14
- Medicare reimbursements for total knee arthroplasty are 5 to 10% lower in states without CON laws, 15 and
- CON laws are associated with higher per-capita Medicaid community-based care expenditures. 16